-I'm sleeping on my repaired side, although I can't tuck my arm in yet. I still leave the arm extended and outwards, away from my body.
-I can now comfortably reach past my left shoulder with my right hand.
-I can dry my back after a shower by holding a towel behind me and pulling back and forth.
-I can reach up with my repaired arm and grab the top of a door frame, unassisted.
-I can throw a frisbee, backhand & forehand, about 5+ yards! (Heather and I tossed this past weekend. I got about 25 throws in before my arm got tired!)
-I am allowed to back squat with the bar (up to this point I wasn't able to even get my arms back behind my head comfortably to hold the bar in place). Worked up to sets of 135 and felt good.
-I am allowed to carry weights in my right arm, now; arm by my side, hanging, only. This is useful for doing weighted lunges and similar lower body exercises.
-My warmups for therapy no longer start with a heating pad, but on the hydraulic arm bike!
-I am doing strengthening exercises with bands and weights now (See more, below)
-I got a parachute for Christmas and am did a kick ass sprint workout with it, last weekend! I'm also getting my cardio fitness back up. I've worked up to eight minutes at ten m.p.h. on the treadmill (~1.3mi).
And now onto the details, if you feel so inclined to read on.
My overhead and external ROM are 80-85%, and that last little bit is in sight. I started this exercise to get over that last hump of stiffness.

In addition, when I get to the top of my ROM I slide over into the door frame forcing my arm up further. By forcing into the door frame, I can also push my lats & teres muscles back into my body, stopping them from (chicken) 'winging'.
As far as ROM, my internal rotation is also getting much better, and I can do this now.

The winging I mentioned above is already much better as I have already gained considerable strength in my teres/scapula from doing weighted table work. From the position in the first image shown, I have worked up to 3 lb. underhand raises (lifting weight in plane with my body, fingers pointing towards my feet), which hits the rhomboids (image 2), and 1 lb. side raises, hitting the deltoids/shoulder and scapula (image 3a). The added motion with the side raises is to get the thumbs pointed as much as possible up towards the ceiling (image 3b), with the idea of helping rotation within the shoulder joint, which I only have about 50% ability to do.

Image 1 - base position

Image 2 - underhand raises, rhomboids

Image 3a - side raises, deltoid, scapula, shoulder etc.

Image 3b - thumbs up!


Abduction


Rows
I'm also working on postural strengthening. This exercise requires a tight core, and arms, elbows, shoulders, back, butt, all against the wall. The trouble I'm having is even though my external rotation in a supine position has reached 80-90 degrees, there is still stiffness in the joint, and full ROM requires assistance by pushing the arm out in that plane of motion. Actively moving my arm against the wall isn't yet possible. Note: I haven't started doing wall slides in the way shown below, yet, although my standard wall slides are becoming much easier and I can now almost fully keep my arms parallel as I do them!

Postural strengthening (left image)
Modification with upward wall slides (right image)

Supine external rotation of the shoulder. When I do my postural strengthening against the wall, this is about as far as I can get my arm, so far.
One of the harder things I am now doing is a side bridge to strengthen the teres major which should help immensely with my aforementioned 'winging'.


Side bridge Teres major
Finally, I'm doing, for lack of a better term, what we call a table lean. The image below is actually meant to demonstrate single-armed incline pushups, but it's the closest thing I could find to what I'm doing. Essentially, I start with both arms on the bench/table/chair in front of me, and alternate between balancing in the 'up' position of the incline pushups, which I'm also using to target the teres, stabilizing the shoulder, but also requires pectoralis, core, and even some groin/glute tightening. What the image doesn't show, is that sinking the hips into the table is required, and the closer the feet are together, the harder this gets to hold.
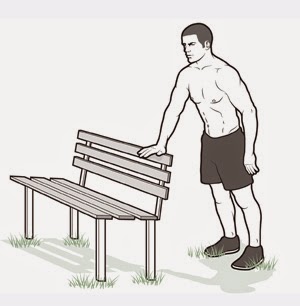
"Table leans"
So the verdict is, after eight weeks, I'm well into phase III (strengthening), again, ahead of schedule. I'm sleeping better. I feel good. I'm doing sprint workouts now! Everything is doing great on this last day of 2014, and I am excited for 2015 to start.
Happy New Year!














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}